The second most common malignant tumor in women after breast tumors is cervical cancer. The pathology occurs in 8-11 women out of 100 thousand. Every year, up to 600 thousand newly discovered cases of the disease are registered around the world.
Signs of cervical cancer most often develop in patients over 40 years of age. The risk of getting sick in this group is 20 times higher than in girls 25 years old. About 65% of cases are found in the age group of 40-60 years, 25% in the group of 60-69 years old. Early stages of pathology are more often detected in women 25-40 years old. In this case, the disease can be easily cured, so it is very important to be regularly examined by a gynecologist.
In Russia, early stages of this pathology are registered in 15% of patients, advanced cases - in 40% of patients who applied for the first time.
Causes and mechanism of development
Cervical carcinoma: what is it? According to the definition of the World Health Organization, it is a malignant tumor that arises from the cells of the layer lining the surface of the organ from the outside, that is, the epithelium.
Modern medicine still does not have enough data to speak with confidence about the etiological factors of the disease. The mechanism of tumor development is also poorly understood. This is largely due to the difficulties of prevention and early detection of cervical tumors.
It is known that the causes of cervical cancer are associated with infection types 16 and 18. Viral infection is detected in 57% of patients.
Social disadvantage and promiscuous sexual relations are important. The harmful effects of smoking have been proven.
The cervix is lined by multilayered epithelium. Its cells are flat in shape and arranged in layers. Under the influence of the virus, the epithelium gradually changes its structure, and malignancy occurs - tissue malignization.
Stages of malignancy:
- Epithelial cells respond to damage by dividing more rapidly to repair damaged tissue.
- Precancerous changes occur, which consist in disruption of the structure of the epithelial layer -.
- Gradually, malignant changes appear in the thickness of the cells: the epithelium begins to divide uncontrollably. Pre-invasive cervical cancer occurs (in situ, or “in place”).
- The malignant tumor then spreads beyond the epithelium and penetrates the stroma - the underlying tissue of the cervix. If this growth is less than 3 mm, they speak of microinvasive carcinoma. This is an early stage of invasive cancer.
- When it grows into the stroma more than 3 mm, invasive cervical cancer occurs. In most patients, external signs and clinical symptoms of the disease appear only in this phase.
Detection of precancerous changes is the basis for early diagnosis and successful treatment of the disease. Dysplasia is accompanied by the proliferation of altered (atypical) cells inside the epithelial layer, while the upper layer does not change and consists of ordinary cells with signs of keratinization.
Carcinoma in situ (pre-invasive or non-invasive cervical cancer) is accompanied by a violation of the layering of the epithelium and the presence of malignant cells throughout its entire thickness. However, the tumor does not grow into the underlying tissue, so it is well treated.
Forms of the disease
The morphological structure of a tumor is the external changes in the shape and structure of its cells. The degree of tumor growth and its malignancy depend on these features. Morphological classification includes the following forms:
- squamous cell keratinizing;
- squamous without keratinization;
- poorly differentiated cancer;
- glandular (adenocarcinoma).
Squamous cell variants occur in 85% of cases, adenocarcinoma – in 15%. Keratinizing cervical cancer has a high degree of cellular maturity and a more favorable course. It is observed in 20-25% of women. The non-keratinizing form with an average degree of differentiation is diagnosed in 60-65% of patients.
Adenocarcinoma predominantly develops in the cervical canal. Poorly differentiated tumors with a high degree of malignancy are rarely diagnosed, so timely diagnosis makes it possible to successfully treat most types of cancer. In 1-1.5% of patients, clear cell, small cell, mucoepidermoid and other tumor variants are detected.
Depending on the direction of tumor growth, the following forms are distinguished:
- with endophytic growth (inward, towards the underlying tissues, with transition to the body of the uterus, appendages, vaginal wall);
- with exophytic growth (into the vaginal lumen);
- mixed.
Clinical manifestations
About 10% of cases of the disease have a “silent” course, that is, they are not accompanied by any external manifestations. Signs of cervical cancer at an early stage can only be detected by examination and cytological examination.
How quickly does the tumor develop?
The transformation of a precancerous condition into cancer takes from 2 to 10 years. If at this time a woman is regularly examined by a gynecologist, the likelihood of recognizing the disease at an early stage is very high. The transition of cancer from stage 1 to stage 2 and subsequent ones takes an average of 2 years.
In later stages, symptoms of cervical cancer appear:
- bloody discharge;
- leucorrhoea;
- pain.
The intensity of bleeding may vary. They are observed in two variants:
- contact: appear during sexual intercourse, vaginal gynecological examination, and also often during defecation;
- acyclic: represent spotting before and after menstrual bleeding and occur in 60% of patients.
A quarter of patients experience light-colored discharge – leucorrhoea. They may be watery or become mucopurulent. They often acquire a foul odor. Leucorrhoea appears due to damage to the lymphatic capillaries during the destruction of dead areas of a malignant neoplasm. If blood vessels are also affected, an admixture of blood is visible in the discharge.
How does cervical cancer manifest itself in the next stage?
Many patients complain of pain in the lower back, sacrum, spreading to the anal area and legs. The pain is associated with compression of the nerve trunks by a tumor that has spread to the pelvic tissue. Pain syndrome also occurs when the pelvic lymph nodes and bones are affected.
When a tumor grows into the wall of the intestine or bladder, constipation, blood in the stool, and frequent painful urination are possible.
When large lymphatic collectors are compressed, swelling of the legs appears. A prolonged slight increase in temperature is possible. Nonspecific manifestations of malignant tumors include weakness and decreased performance.
Main complications requiring immediate hospitalization and treatment:
- intense bleeding from the vagina;
- intestinal obstruction;
- acute renal failure;
- severe pain syndrome.
Diagnostics
To recognize a cervical tumor, doctors analyze the patient’s life history and illness, and conduct laboratory and instrumental studies. A comprehensive diagnosis of cervical cancer is necessary to clarify the stage and determine an individual treatment plan.
Life history features that increase the likelihood of a tumor:
- early sexual life;
- multiple sexual partners;
- infectious diseases transmitted through sexual contact;
- abortions;
- cervical injury during childbirth;
- previous biopsy, diathermocoagulation or diathermoconization;
The basis of early diagnosis is an annual preventive medical examination of women with mandatory superficial scraping from the cervix and its cytological examination. Cytological analysis allows you to clearly examine epithelial cells under a microscope and detect precancerous or malignant changes.
Cytological screening should be carried out in all women from the age of 18-20 years. It is enough to perform it once every 3 years, however, with an annual examination, the frequency of detecting a malignant tumor at an early stage increases. Smear analysis gives a reliable result in 90-98% of cases, and erroneous conclusions are most often false positive. Cases where an existing tumor is not recognized by cytological examination are extremely rare.
What is the test for cervical cancer called?
In many countries, cytological screening using Papanicolaou is used; in Russia, a modification of this method is used. It begins 3 years after the start of sexual activity or upon reaching the age of 21. You can stop the screening test in women over 70 years of age with an unchanged cervix and at least three negative smear results over the past 10 years.
If precancerous changes (dysplasia) are detected, the woman undergoes an in-depth examination.
How to determine cervical cancer at the second diagnostic stage?
The following methods are used for this:
- gynecological examination;
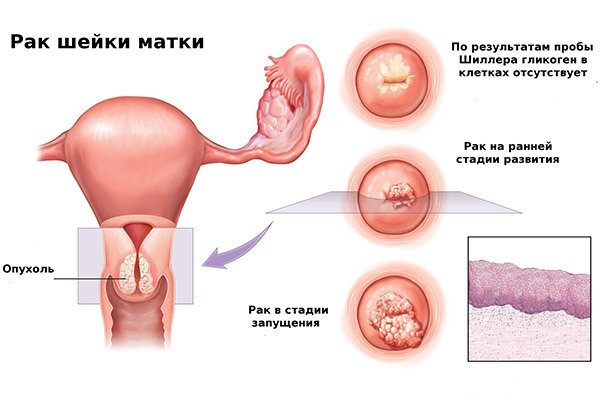
- with Schiller's test (examination of the cervix under a special microscope with staining of its surface with Lugol's solution); areas of pathologically altered epithelium are not stained during the Schiller test, which helps the doctor take a biopsy from the lesion;
- repeated cytological and histological studies.
A complete examination allows a diagnosis to be made in 97% of patients.
Additional diagnostic methods
A tumor marker for cervical cancer, the specific antigen SCC, is examined in the patients’ blood. Normally, its concentration is no more than 1.5 ng in 1 ml. In 60% of patients with squamous cell carcinoma, the level of this substance is elevated. Moreover, their likelihood of relapse is 3 times higher than in patients with normal SCC. If the antigen content is more than 4.0 ng in 1 ml, this indicates metastatic damage to the pelvic lymph nodes.

Colposcopy is one of the main methods used to identify a tumor. This is an examination of the cervix using an optical instrument that provides a magnification of 15 times or more. The examination makes it possible to identify areas of pathology in 88% of cases and take a targeted biopsy. The examination is painless and safe.
The information content of only cytological diagnosis of a smear without a biopsy is 64%. The value of this method increases with repeated analyses. The study does not make it possible to distinguish between preinvasive and invasive types of tumor, so it is supplemented with a biopsy.
If changes are detected using histological and cytological examination, as well as during colposcopy, an extended biopsy of the cervix is prescribed - conization. It is performed under anesthesia and involves excision of cervical tissue in the form of a cone. Conization is necessary to assess the depth of tumor penetration into the underlying tissue. Based on the results of the biopsy, doctors determine the stage of the disease, on which treatment tactics depend.
After analyzing the clinical data and the results of additional diagnostics, the doctor should receive an answer to the following questions:
- whether the patient has a malignant tumor;
- what is the morphological structure of cancer and its spread to the stroma;
- if there are no reliable signs of a tumor, are the detected changes precancerous;
- Is the data obtained sufficient to exclude the disease?
To determine the spread of the tumor to other organs, radiation methods for recognizing the disease are used: ultrasound and tomography.
Is cervical cancer visible on ultrasound?
You can detect a tumor that has spread into its thickness or into the wall of surrounding organs. This study is not carried out to diagnose education at an early stage. On ultrasound, in addition to changes in the organ itself, damage to the pelvic lymph nodes is visible. This is important for determining the stage of the disease.
Additionally, studies aimed at identifying distant metastases are prescribed:
- X-ray of the lungs;
- excretory urography;
- cystoscopy;
- rectoscopy;
- lymphography;
- bone scintigraphy.
Depending on the accompanying symptoms, the patient is referred for consultation to one or more specialists:
- cardiologist;
- gastroenterologist;
- neurosurgeon;
- thoracic surgeon;
- endocrinologist
Doctors of the listed specialties identify metastases in distant organs and also determine the safety of surgical treatment.
Classification
For the most successful treatment, the doctor needs to determine the extent of the tumor, the extent of damage to the lymph nodes and distant organs. For this purpose, two classifications are used, largely repeating each other: the TNM system (“tumor – lymph nodes – metastases”) and FIGO (developed by the International Federation of Obstetricians and Gynecologists).
- T – tumor description;
- N0 – regional lymph nodes are not involved, N1 – metastases in the pelvic lymph nodes;
- M0 – there are no metastases in other organs, M1 – there are tumor foci in distant organs.
Cases where diagnostic data are not yet sufficient are designated Tx; if the tumor is not detected - T0. Carcinoma in situ, or non-invasive cancer, is designated Tis, which corresponds to FIGO stage 0.
There are 4 stages of cervical cancer
Stage 1 FIGO cancer is accompanied by the appearance of a pathological process only in the cervix itself. There may be such damage options:
- invasive cancer, determined only microscopically (T1a or IA): penetration depth up to 3 mm (T1a1 or IA1) or 3-5 mm (T1a2 or IA2); if the depth of invasion is more than 5 mm, the tumor is classified as T1b or IB;
- tumor visible upon external examination (T1b or IB): up to 4 cm in size (T1b1 or IB1) or more than 4 cm (T1b2 or IB2).
2 stage accompanied by tumor spread to the uterus:
- without germination of periuterine tissue, or parametrium (T2a or IIA);
- with germination of the parametrium (T2b or IIB).
3 stage cancer is accompanied by the proliferation of malignant cells in the lower third of the vagina, pelvic walls or kidney damage:
- affecting only the lower part of the vagina (T3a or IIIA);
- with involvement of the pelvic wall and/or kidney damage leading to hydronephrosis or a non-functioning kidney (T3b or IIIB).
Stage 4 accompanied by damage to other organs:
- with damage to the urinary system, intestines or tumor extension beyond the pelvis (T4A or IVA);
- with metastases in other organs (M1 or IVB).
To determine the extent of lymph node involvement, examination of 10 or more pelvic lymph nodes is necessary.
The stages of the disease are determined clinically, taking into account data from colposcopy, biopsy, and examination of distant organs. Methods such as CT, MRI, PET or lymphography are only of additional value for staging. If there is doubt about staging, the tumor is classified as a milder stage.
Treatment Methods

For patients with early-stage tumors, cervical cancer is treated with radiation or surgery. The effectiveness of both methods is the same. In young patients, it is better to use an operation after which the function of the ovaries and uterus is not impaired, atrophy of the mucous membrane does not develop, and pregnancy and childbirth are possible.
There are several options for how to treat cervical cancer:
- surgery only;
- combination of radiation and surgery;
- radical radiotherapy.
Surgical intervention
Removal of the uterus and appendages can be performed using. The method allows you to avoid extensive incisions, trauma to internal organs and the formation of adhesions. The duration of hospitalization for laparoscopic surgery is significantly less than for traditional surgery and is 3-5 days. Additionally, vaginal plastic surgery can be performed.
Radiotherapy
Radiation therapy for cervical cancer can be given before surgery using a fast-track technique to reduce the size of the tumor and make it easier to remove. In many cases, surgery is performed first, then the tissue is irradiated to destroy any remaining cancer cells.
If surgery is contraindicated, a combination of external and intracavitary radiotherapy is used.
Consequences of radiation therapy:
- atrophy (thinning and dryness) of the vaginal mucosa;
- infertility due to concomitant ovarian damage;
- due to inhibition of hormonal activity of the gonads, a few months after irradiation may occur;
- in severe cases, communications may form between the vagina and adjacent organs. Fistulas may leak urine or feces. In this case, surgery is performed to restore the vaginal wall.
The treatment program is developed individually, taking into account the stage and size of the tumor, the general condition of the woman, damage to the pelvic lymph nodes and other factors.
Chemotherapy
Adjuvant (postoperative) chemotherapy with Fluorouracil and/or Cisplatin is often used. Chemotherapy may be given before surgery to reduce the size of the tumor. In some cases, chemotherapy is used as an independent treatment method.
Modern methods of treatment:
- targeted therapy using agents of biological origin; such drugs accumulate in tumor cells and destroy them without damaging healthy tissue;
- intravaginal antiviral therapy;
- photodynamic treatment: a light-sensitive drug is injected into the tumor, and with subsequent laser exposure, the tumor cells disintegrate;
- IMRT therapy is intensity-modulated radiation that allows you to gently target the tumor without damaging healthy cells;
- brachytherapy – introduction of a radiation source in close proximity to the tumor site.
Nutrition
At home, the patient must adhere to a certain diet. Nutrition should be complete and varied. Of course, diet cannot defeat cancer. However, the beneficial effects of the following products cannot be ruled out:
- carrots, rich in plant antioxidants and carotenoids;
- beet;
- green tea;
- turmeric.
A variety of vegetables and fruits, as well as sea fish, are useful. It is not recommended to consume the following products:
- refined carbohydrates, sugar, chocolate, carbonated drinks;
- canned foods;
- spices;
- fatty and fried foods;
- alcohol.
At the same time, it is worth understanding that with stage 3-4 cancer, patients’ life span is often limited, and a varied diet helps them improve their psychological state.
Rehabilitation period
Recovery after a course of treatment includes a gradual increase in physical activity. Elastic leg bandaging is used to prevent venous thrombosis. After the operation, breathing exercises are indicated.
The support of loved ones is important. Many women need help from a medical psychologist. After consulting with a doctor, you can use some herbal remedies, but many experts are wary of this method of treatment, because the safety of herbs for cancer has practically not been studied.
A woman's health usually recovers within a year. During this period, it is very important to avoid infections, physical and emotional stress.
Features of treatment of cervical cancer depending on stage
Non-invasive cancer
Non-invasive cancer is an indication for cervical conization. It can be performed using a scalpel, as well as electricity, laser or radio waves. During the intervention, the altered cervical tissue is removed in the form of a cone, directed with its apex upward, towards the internal os of the uterus. The resulting material is carefully examined to ensure complete removal of a small malignant lesion.
Another surgical option is trachelectomy. This is the removal of the cervix, adjacent part of the vagina and fatty tissue, pelvic lymph nodes. Such intervention helps preserve the ability to bear children.
If the tumor has spread along the cervical canal to the internal os and/or in elderly patients, it is preferable to remove the uterus and appendages. This can significantly improve the prognosis for life.
In rare cases, due to severe illness, any surgical interventions are contraindicated. Then, to treat carcinoma in situ, intracavitary radiation therapy is used, that is, radiation using a source inserted into the vagina.
IA stage
In case of stage IA cancer, when the depth of germination into the underlying tissue is less than 3 mm, if the patient insists on maintaining the ability to bear children, conization of the cervix is also performed. In other cases, patients before menopause have their uterus removed without the appendages in order to maintain natural hormonal levels. For elderly women, extirpation of the uterus and appendages is indicated.
During the intervention, the pelvic lymph nodes are examined. In most cases they are not removed. In 10% of patients, metastases are noted in the pelvic lymph nodes, then they are removed.
With a tumor penetration depth of 3 to 5 mm, the risk of spread to the lymph nodes increases sharply. In this case, removal of the uterus, appendages and lymph nodes (lymphadenectomy) is indicated. The same operation is performed when the depth of cancer cell invasion is unclear, as well as if tumor recurrence occurs after conization.
Surgical treatment is supplemented with intracavitary radiotherapy. If the germination depth is more than 3 mm, a combination of intracavitary and external irradiation is used. Intensive radiation therapy is also carried out if it is impossible to perform surgery.
Tumors IB-IIA and IIB-IVA stages
For stage IB-IIA tumors up to 6 cm in size, either extirpation of the uterus, appendages and lymph nodes, or intensive radiation therapy is performed. Using each of these methods, the 5-year survival rate for cervical cancer reaches 90%. For adenocarcinoma or a tumor larger than 6 cm, surgical and radiation intervention is combined.
Stage IIB-IVA cancer is not usually treated with surgery. However, in many cases, the stage of the tumor can only be determined during surgery. In this case, the uterus, appendages, and pelvic lymph nodes are removed and postoperative radiotherapy is prescribed.
Another treatment option: external beam radiation, brachytherapy (injecting a radiation source into the tissue of the cervix) and chemotherapy are first prescribed. If a good effect is achieved, a Wertheim operation is performed for cervical cancer (removal of the uterus, appendages and lymph nodes). Radiation therapy is then resumed. To improve the patient's condition, preliminary movement (transposition) of the ovaries is possible. Then they are not exposed to the harmful effects of radiation and retain the ability to produce sex hormones.
Relapses of the disease usually occur within 2 years after surgery.
IVB stage
If the patient has distant metastases, none of the operations leads to a significant improvement in quality of life and prognosis. Radiation therapy is prescribed to reduce the size of the tumor lesion and eliminate compression of the ureters. When cancer recurs, especially if the newly appeared lesion is small, intensive radiation helps to achieve life preservation for 5 years within 40-50%.
IIB-IVB stages
In these cases, chemotherapy may be prescribed after radiation. In stage 4, its effectiveness has been little studied. Chemotherapy is used as an experimental method of treatment. How long do patients with distant metastases live? Once diagnosed, life expectancy is on average 7 months.
Treatment during pregnancy
If a woman is diagnosed with cervical cancer during pregnancy, treatment is determined by the stage of the tumor.
At stage 0 in the first trimester, the pregnancy is terminated and conization of the cervix is performed. If a tumor is detected in the second or third trimester, the woman is regularly examined, and 3 months after birth, conization is performed. In this case, radiosurgery with the Surgitron or Visalius apparatus is often used. This is a gentle treatment method.
If stage 1 cancer is diagnosed during pregnancy, there are 2 options: either termination of pregnancy, removal of the uterus and appendages, or pregnancy followed by surgery and radiation according to the standard regimen. In cases of 2 or more severe stages, the pregnancy is terminated in the first and second trimesters, and a caesarean section is performed in the third trimester. Then the standard treatment regimen is started.
If the patient has undergone organ-preserving treatment, she is allowed to become pregnant 2 years after completion of therapy. Childbirth is carried out only by caesarean section. After the illness, the frequency and perinatal mortality in children increases.
Prognosis and prevention
A malignant tumor of the cervix is a serious disease, but with early diagnosis it can be successfully cured. At stage 1, survival rate over five years is 78%, at stage 2 - 57%, at stage 3 - 31%, at stage 4 - 7.8%. Overall survival rate at five years is 55%.
After the course of treatment, patients should be regularly monitored by a gynecologist. During the first 2 years, analysis for SCC, ultrasound, and, if necessary, CT is carried out once a quarter, over the next 3 years - once every six months. X-ray of the lungs is performed 2 times a year.
Taking into account the great social significance of the disease and the unfavorable prognosis in advanced cases, prevention of cervical cancer is very important. You should not neglect annual visits to the gynecologist, because they can save the health and life of a woman.
Prevention measures:
- Regular observation by a gynecologist, starting from 18-20 years of age, with mandatory cytological screening.
- Early diagnosis and treatment of cervical diseases.
The incidence of the disease is gradually decreasing. However, there is a noticeable increase in incidence in women under 29 years of age. This is largely due to women's limited knowledge about risk factors for the disease. To reduce the likelihood of precancerous pathology, early initiation of sexual activity and infections transmitted through sexual contact should be avoided. Condoms help to significantly reduce, although not eliminate, the likelihood of infection with the papilloma virus.
In order to develop immunity to the virus, it is indicated to prevent precancerous and cancerous diseases of the cervix, as well as genital warts.